
What will the Food and Drug Administration look like under Martin "Marty" Makary, a Johns Hopkins surgeon, President Trump's soon-to-be confirmed commissioner of the Food and Drug Administration (FDA)? FDA-regulated industries — which produce goods representing some 25 cents of every consumer dollar — are bracing for possible changes in drug, device, biologics and food regulation. While specific priorities are not year clear, history and recent trends provide key areas to watch.
Who's really in charge?
A little-known fact is that the ultimate authority for all the FDA approvals – drugs, biologics, medical devices, food additives, and so on technically resides with the Secretary of Health and Human Services, who then routinely delegates individual decisions to the FDA Commissioner, who, in turn, may delegate approval authority farther down the food chain. In other words, even if Makary advocates somewhat rational FDA policies — not a given under this administration — he ultimately takes his marching orders from Robert F. Kennedy, Jr., the delusional, science-challenged, anti-vaccine activist and "chemtrails" conspiracy theorist. RFK, Jr. could arbitrarily interdict FDA approvals he didn't like. Responsible also for overseeing other agencies, including the CDC, NIH, and Centers for Medicare and Medicaid Services, Kennedy would be a clear and present danger to the health of Americans.
In fact, there may not be significant divergence between policies advocated by RFK, Jr. and Makary. He too repeatedly expressed dubious opinions during the COVID-19 pandemic. He contended that public health officials pursued overly harsh vaccination mandates and ignored alternative strategies, such as the "natural immunity" conferred by infections. He was part of a misguided group of physicians who called for greater emphasis on herd immunity to end the pandemic and promoted the dangerous idea that mass infections would quickly lead to population-level protection. That turned out to be a catastrophic recommendation as the virus mutated so quickly and such dramatic fashion that herd immunity was impossible to achieve. As a result, predictions by Makary and other signees to the Great Barrington Declaration that as few as 20,000 people in the US were likely to die from COVID infections ended up being off by 1.3 million — a mere 6,400%.
Makary has also criticized the supposed overprescribing of drugs, the use of pesticides on foods, and the alleged undue influence of pharmaceutical and insurance companies over doctors and government regulators.
Regulatory trends
In the broader regulatory landscape, ongoing activities like drug application reviews and inspections are expected to continue. However, some high-profile initiatives — such as the regulation of laboratory-developed tests (LDTs) and digital health products — may face delays or revision as the new administration's policy preferences become clearer.
In 2024, the FDA made strides in the regulation of drugs and biologics, including finalizing a pathway for approving nonprescription drugs with added safety measures, known as Additional Conditions for Nonprescription Use (ACNUs). This regulatory framework aims to expand consumer access to Over the Counter (OTC) drugs while ensuring safety. As 2025 unfolds, the industry will closely monitor how the FDA and individual manufacturers implement these changes.
Advanced manufacturing technologies have also been a high priority. The FDA's "new platform technology" designation program is intended to streamline the regulatory process for innovative manufacturing techniques. Similarly, the Advanced Manufacturing Technologies Designation Program seeks to incentivize the adoption of novel manufacturing processes. These initiatives are expected to continue evolving, reflecting the FDA's commitment to modernizing drug production.
Republican administrations have historically been inclined to reduce regulatory burdens. During President Trump's previous term, for example, the FDA attempted to reclassify certain medical devices to exempt them from premarket clearance requirements and proposed expanding the category of drugs that could be marketed without FDA approval. Similar deregulatory efforts may resurface, potentially altering the landscape for device manufacturers and pharmaceutical companies.
Independent of the upheavals wrought by the Trump victory, the 2024 Supreme Court decision in Loper Bright will steer policy in a still unclear direction. The Chevron doctrine had granted agencies considerable deference in interpreting their authorities. With the shift to judicial oversight, the review of new rules and regulatory decisions now falls to judges who usually have little or no expertise in what they are assessing; most lack the specialized knowledge that agencies bring to the table in fast-evolving technologies like artificial intelligence (AI) and genetic engineering that are accelerating the development of new drugs, biologics and medical devices.
This decision is likely to reverberate across FDA policymaking and enforcement. Legal challenges to FDA actions, ranging from drug compounding to exclusivity determinations, have already invoked Loper Bright. Without the requisite expertise, judges tasked with ruling on the legality of new rules and regulatory decisions will inevitably make some fragmented, inconsistent decisions that vary across jurisdictions.
As these cases proceed through the courts, the FDA may need to adapt its practices to conform to the new judicial dictates. And there is a broader fear that the overturning of Chevron undermines the role of science in US rulemaking, as it shifts the burden of interpreting ambiguous laws from federal agencies to courts and special interests, potentially hindering science-based regulation and public health protections.
Policy
Artificial intelligence (AI) and digital health are likely to remain central to FDA's agenda. Early 2025 has already seen the release of draft guidance on the use of AI in regulatory decision-making for drugs and biologics. The application of AI to medical product development also offers transformative potential, but questions remain about how evolving regulatory frameworks will address these technologies under the new administration.
In 2024, the FDA issued guidance on misinformation related to medical devices and prescription drugs, highlighting the importance of ensuring accurate product information for healthcare providers and patients. While this initiative aligns with longstanding FDA priorities, its specific framing around misinformation may reflect the outgoing administration's focus. How the new leadership approaches this issue will signal its broader communication strategy. Unfortunately, the FDA Commissioner-designate, Dr. Makary, was himself a prominent spreader of medical misinformation during the past four years. His pairing with Robert F. Kennedy, Jr., a serial and dedicated purveyor of dangerous medical misinformation, is ominous.
The FDA's user fee programs, which fund significant portions of its operations via fees paid by regulated industry, are entering a critical phase. The Over the Counter (OTC) monograph user fee program requires reauthorization by Congress by September 2025, while negotiations for reauthorizing major user fee programs for drugs, biologics, and medical devices are set to begin. These discussions will shape the agency's resources and priorities for years to come, but the Trump administration brings uncertainty. During his first term, President Trump attempted to double user fees to speed up drug approvals, but these plans were eventually shelved. The administration's potential influence on the FDA's negotiations with the pharmaceutical industry could include executive orders or other measures to dictate the agency's position.
Beyond user fees, the new administration may explore broader policy changes affecting the life sciences industries. Topics like drug pricing, supply chain resilience, and international harmonization of regulatory standards could gain prominence, depending on the administration's priorities.
Impact on employees
The White House has announced the firing of thousands of Department of Health and Human Services employees at the FDA, CDC, and other agencies, according to reporting by the New York Times. A New York Times article contained this masterpiece of understatement:
The agencies are responsible for a range of functions, from approving new drugs to tracing bird-flu outbreaks and researching cancer. A loss of staff could affect the efforts depending on which workers are cut and whether they are concentrated in particular areas.
The Trump administration has also offered the majority of the federal government's three million employees a "buyout" via a "deferred resignation program" that would put them on paid administrative leave through September, after which their employment would be terminated. To encourage them to accept the offer, the notice included a warning that "the majority of federal agencies are likely to be downsized through restructurings, realignments, and reductions in force."
A problem with such a plan is that the federal employees who are accepting the offer tend to be the most capable and most employable in the federal workforce, thus enriching for the less talented "lifers" who remain. This hardly seems a sound strategy for improving the efficiency and effectiveness of federal agencies throughout the government.
A slew of long-term FDA civil-service employees are also likely to leave voluntarily or be forced out. Others will leave because of the recent executive order mandating that federal employees return to offices, which will require FDA staff to work from the agency's White Oak headquarters, regional offices or duty stations. Many federal employees have relocated far from their government offices and would suffer severe inconvenience or expense to return. Such resignations are costly to federal agencies, in terms of both efficiency and resources, because of the need to train replacements and bring the new arrivals up to speed on the arcana of federal regulations and procedures.
A reminder, although it should be obvious: The displacement of federal employees who have arcane expertise at agencies whose approval is required before new life-saving drugs and medical devices can be marketed benefits no one.
The dislocations extend to the very top of the FDA's leadership. The Center for Drug Evaluation and Research (CDER) and the Center for Biologics Evaluation and Research (CBER) have already experienced leadership changes. Notable departures include Dr. Patrizia Cavazzoni, former CDER Center Director, and Dr. Celia Witten, CBER Deputy Center Director. These transitions could lead to significant shifts in priorities within these critical divisions.
Regulatory changes, challenges and opportunities
The transitional period following an election is also undoubtedly delaying the publication of new regulations, guidance documents and other important notices. Another unknown during this transition is the impact of the promised sharp reduction in the numbers of federal civil servants. At agencies like the FDA where affirmative approvals of most products must be granted for them to be marketed, fewer reviewers, inspectors, and administrators could lead to prolonged approval times. That will benefit no one.
The new Administration's deregulation plans are ambitious but murky. According to the government's January 31 Executive Order: "Overregulation stops American entrepreneurship, crushes small business, reduces consumer choice, discourages innovation, and infringes on the liberties of American citizens." The accompanying White House Fact Sheet states that "the Order requires that whenever an agency promulgates a new rule, regulation, or guidance, it must identify at least 10 existing rules, regulations, or guidance documents to be repealed."
The problem with that "quota" is the definition of what triggers the 10-for-1 policy. It counts any "agency statement of general or applicability and future effect designed to implement, interpret, or prescribe law or policy or to describe the procedure or practice requirements of an agency, including, without limitation, regulations, rules, memoranda, administrative orders, guidance documents, policy statements, and interagency agreements. (Emphasis added.)
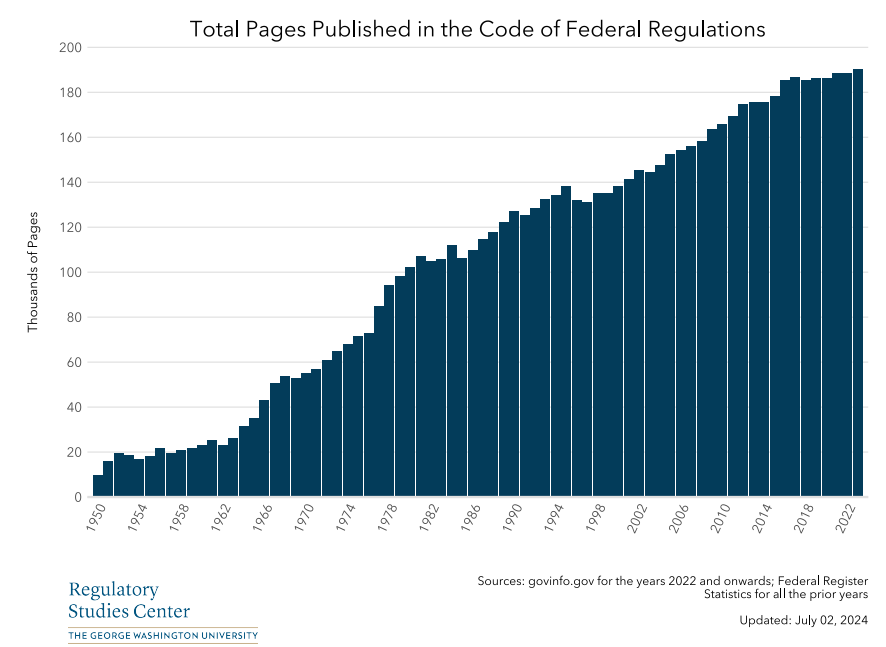
At an agency like the FDA, which regulates some 25 cents of every consumer dollar, that definition could encompass dozens of such "statements" every week, many of which streamline or clarify regulation, announce the approval of new products, or warn of recalls of contaminated or otherwise dangerous products. Safely repealing ten times the number of such statements would is impossible. This illustrates the danger of cutting with a meat cleaver when what's needed is a scalpel.
The interplay among political leadership, regulatory priorities, and industry innovation will define the FDA's trajectory under the new administration. While some changes may streamline processes and foster innovation, others could slow progress or introduce uncertainty in key areas. Collaboration among regulators, industry, public interest groups, and other stakeholders will be essential to ensure that regulatory frameworks protect public health while supporting innovation. It won't be an easy task.
Henry I. Miller, a physician and molecular biologist, is the Glenn Swogger Distinguished Fellow at the American Council on Science and Health. A 15-year veteran of the FDA, he was the founding director of its Office of Biotechnology.