
In spite of the surging number of new cases of COVID-19 in many U.S. hot spots, worrisome increases in the percentage of positive tests, and scores of intensive-care units at or near capacity, some (mostly conservative) pundits and politicians seem not to "get it." They parrot talking points that seem intended to divert attention from serious issues by burying their audience with arcane and irrelevant statistics.
For a while, as the body count climbed, some conservative commentators insisted there is "a big difference between dying from the virus and dying with the virus." Then they shifted to quibbling over the discrepancies between when a death occurred and when it was reported.
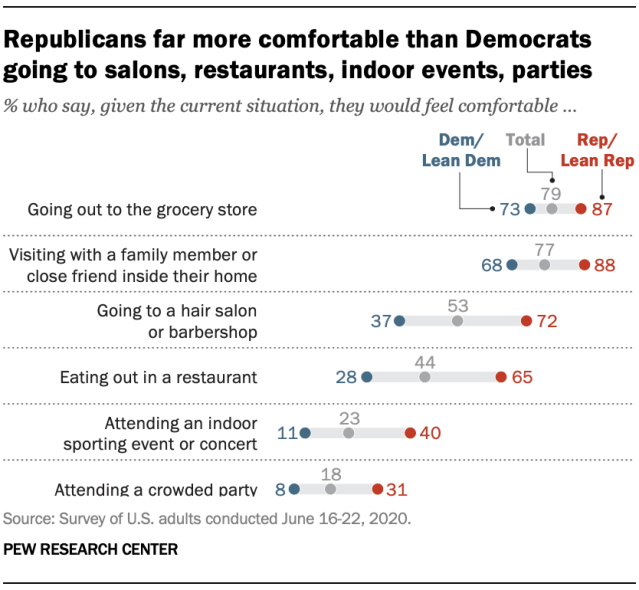
Thereby, the punditocracy seems to have persuaded many Republicans to be less concerned than Democrats about COVID-19 infection, according to a Pew Research Center poll:
Republican Sen. Ron Johnson of Wisconsin trotted out some newer themes in a recent Wall Street Journal op-ed, the punchline of which was that we don't now need another huge economic stimulus bill from Congress.
I don't have a problem with his conclusion, but the reasoning he used was sophistic, and omitted essential parts of the story. For example, he cited a recent study in JAMA Internal Medicine that measured antibodies in blood to SARS-CoV-2 (the virus that causes COVID-19) which showed that the number of COVID-19 infections in the population – the penetrance – was six to 24 times the number of symptomatic "reported cases." That was hardly a surprise; we've known for months that the majority of COVID-19 infections are asymptomatic and are never diagnosed.
But, critically, Johnson failed to mention the downside of those findings: As the authors of the study noted, "The findings may reflect the number of persons who had mild or no illness or who did not seek medical care or undergo testing but who still may have contributed to ongoing virus transmission in the population" (emphasis added).
That observation has important implications for the conundrum of when schools can be reopened safely: In locales that have large numbers of new cases of COVID-19 infections and high rates of testing positivity, it would be dangerous to have children congregating in classrooms, cafeterias, and gyms. (Children older than 10 spread COVID-19 infections as well as adults, while those under 10 spread it about half as effectively.)
To be clear, if there is widespread COVID-19 in the community, it is likely that children in school will infect their classmates, teachers, school support staff, and relatives, who will then go on to further spread the virus. As Dr. Anthony Fauci has pointed out repeatedly, people harboring asymptomatic COVID-19 are a critical link in the transmission of infections in the community.
Johnson then shifted to discussing COVID-19 fatality rates, comparing them to those from the seasonal flu. Because they don't differ appreciably, he concluded that, therefore, "there is no need to continue broad economic shutdowns with fatality rates in these ranges."
Not so fast, Senator; there's much more to pandemic statistics than fatality rates. For one thing, the absolute number of fatalities this year (around 147,000, as of July 27) is already more than four times the yearly average from seasonal flu.
Case counts are also important. The protean manifestations of COVID-19 and its sequelae in many patients who have "recovered" make it more ominous than a usually transient, flu-like respiratory infection. Although it often presents with pulmonary symptoms and can cause severe pneumonia and "post-COVID pulmonary fibrosis," there have been numerous reports of non-respiratory signs and symptoms, including loss of sense of smell or taste, confusion and cognitive impairments, fainting, sudden muscle weakness or paralysis, abnormal blood-coagulation tests, blood clots, seizures, ischemic strokes, kidney damage, and, rarely, a severe pediatric, multi-organ inflammatory syndrome.
Recovery is often incomplete, with various symptoms persisting after the acute infection has subsided. A recent article in the journal JAMA found in a small study that 87.4% of patients who had recovered from COVID-19 reported persistence of at least one symptom, most often fatigue or dyspnea (i.e., shortness of breath) two months after recovery. The frequency of post-acute COVID-19 symptoms is shown here:

Credit: A Carfi et al, https://jamanetwork.com/journals/jama/fullarticle/2768351?appId=scweb
Extrapolating those findings to the U.S. and making certain conservative assumptions, Dr. Bob Morris estimates the frequency of symptoms in the U.S. would translate to these shocking statistics for COVID-19 patients discharged from hospitals as of July 19:
| Symptom | US Cases |
| Any | 507,000 |
| Fatigue | 308,000 |
| Difficulty Breathing | 252,000 |
| Joint Pain | 158,000 |
| 3 or More | 319,000 |
Those two figures, along with the finding that almost nine in 10 of people who had recovered from COVID-19 reported persistence of at least one symptom two months later, illustrate the fallacy in focusing on fatality rates.
Possibly overlapping with Morris' "three or more category," above, are reports of patients experiencing long-term adverse effects that resemble a condition variously known as myalgic encephalomyelitis or chronic fatigue syndrome (ME/CFS). Its signs and symptoms may include fatigue, loss of memory or concentration, sore throat, swelling of neck or armpit lymph nodes, unexplained muscle or joint pain, headaches, non-restorative sleep, and extreme exhaustion that lasts more than 24 hours after physical exercise or mental stimulation ("post-exertional malaise").
People with ME/CFS are often incapable of performing ordinary activities, and sometimes become completely debilitated, unable even to get out of bed. A good word picture was provided in an interview of three COVID-19 patients on NPR's July 11 "Weekend Edition," who described in poignant terms their ongoing symptoms, and CNN anchor Chris Cuomo recently described on-air experiencing some of these symptoms following his bout with COVID-19.
The manifestations of the syndrome can persist for years, although, of course, we can't yet know what the typical, long-term post-COVID-19 course will be. What we do know is that in recent decades, outbreaks of other infectious diseases, including Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) (both of which are also caused by coronaviruses), as well as West Nile virus, H1N1 influenza, and Ebola — have been followed by a range of long-term complaints that resemble those of ME/CFS. Therefore, it's no surprise to see this phenomenon repeated in COVID-19 patients.
The appearance of serious, persistent COVID-19 sequelae has important implications.
First, fatalities aside, the increase in cases and the high numbers of hospitalizations in epicenters of infection cannot be dismissed as simply a self-limited, "flu-like illness" whose effects are done and gone in a week or so. We need, therefore, to aggressively suppress and mitigate COVID-19. The fewer new cases, the fewer lingering illnesses there will be, with all their attendant misery and expense. (A corollary is that "COVID parties" are dangerous, antisocial, and colossally stupid.)
Second, the persistence of debilitating symptoms argues strongly against vaccine "challenge trials," in which infectious SARS-CoV-2 virus is intentionally administered to test subjects, some of whom have received a trial vaccine while others have gotten a placebo. In the absence of highly effective drugs to treat COVID-19, such studies would arguably be unethical.
Finally, we need research on the long-term effects of COVID-19, so that we can better understand the pathophysiology of both the acute viral infection and the persistent post-infection sequelae. A research group at the NIH's National Institute for Neurological Diseases and Stroke is preparing to enroll patients in a study that will investigate possible aberrations in the immune systems of "long-haulers," people who have persistent symptoms after recovering from COVID-19, but we need much more.
The sad truth is that in terms of both the spread of infections and an understanding of COVID-19's pathophysiology, we are still in the early days of this pandemic. Cherry-picking data to make political points and support flawed policies will only prolong it.
Henry I. Miller, a physician and molecular biologist, was a research fellow at the National Institutes of Health and the founding director of the Office of Biotechnology at the FDA.